Is it possible to introduce an interview to the Korean Medical Licensing Examination to assess professional attributes?: a survey-based observational study
Article information

Abstract
Purpose
This study aimed to gather opinions from medical educators on the possibility of introducing an interview to the Korean Medical Licensing Examination (KMLE) to assess professional attributes. Specifically following topics were dealt with: the appropriate timing and tool to assess unprofessional conduct; the possiblity of prevention of unprofessional conduct by introducing an interview to the KMLE; and the possibility of implementation of an interview to the KMLE.
Methods
A cross-sectional study approach based on a survey questionnaire was adopted. We analyzed 104 pieces of news about doctors’ unprofessional conduct to determine the deficient professional attributes. We derived 24 items of unprofessional conduct and developed the questionnaire and surveyed 250 members of the Korean Society of Medical Education 2 times. Descriptive statistics, cross-tabulation analysis, and Fisher’s exact test were applied to the responses. The answers to the open-ended questions were analyzed using conventional content analysis.
Results
In the survey, 49 members (19.6%) responded. Out of 49, 24 (49.5%) responded in the 2nd survey. To assess unprofessional conduct, there was no dominant timing among basic medical education (BME), KMLE, and continuing professional development (CPD). There was no overwhelming assessment tool among written examination, objective structured clinical examination, practice observation, and interview. Response rates of “impossible” (49.0%) and “possible” (42.9%) suggested an interview of the KMLE prevented unprofessional conduct. In terms of implementation, “impossible” (50.0%) was selected more often than “possible” (33.3%).
Conclusion
Professional attributes should be assessed by various tools over the period from BME to CPD. Hence, it may be impossible to introduce an interview to assess professional attributes to the KMLE, and a system is needed such as self-regulation by the professional body rather than licensing examination.
Introduction
Background/rationale
In recent years in Korea, the media has often exposed the unprofessional conduct of doctors. Korean doctors are allowed to practice after medical school graduation and pass the Korean Medical Licensing Examination (KMLE), and they can practice for a lifetime after completing the continuing medical education for at least 8 hours a year. The public demanded that assessing the humanity or virtue of doctors be added to the KMLE to prevent the unprofessional conduct of doctors. Even a member of the National Assembly insisted on the need to introduce an interview to the KMLE [1]. Literature shows that humanity or virtue is hard to assess, especially as a single examination [2,3]. However, professional attributes can be taught and evaluated continuously [4-7]. Therefore, medical educators focused on professional conduct or attributes [4,5]. Furthermore, to the best of our knowledge, there are no reports of an interview in the licensing exam in the literature from PubMed, Web of Science Core Collection, Scopus, and KoreaMed.
Objectives
This study seeks to gather opinions from medical educators regarding the possibility of assessing professional attributes through an interview in the KMLE. Specific research questions are (1) the appropriate timing, (2) the appropriate tool to assess unprofessional conduct, (3) the possibility of an interview to prevent future unprofessional conduct, and (4) the possibility of implementing an interview to assess professional attributes in the KMLE.
Methods
Ethics statement
This study was approved by the Institutional Review Board of Inje University (approval no., 118.038.025.149). Informed consent was obtained from participants.
Study design
This was a survey-based observational study. It was described according to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) Statement (https://www.strobe-statement.org/).
Setting
The survey was conducted for 2 months, from February to March 2020. The survey was sent twice, and it was conducted via e-mail. In the second e-mail survey, we added one question about the possibility of implementing an interview to assess professional attributes in the KMLE.
Participants
The survey subjects were 250 members (as of December 2019) of the Korean Society of Medical Education. The first survey respondents were 57, and the second survey respondents were 24. The 37 responses that did not respond to appropriate timing or tool to assess unprofessional conduct were excluded.
Variables
The 4 main variables of interest were (1) the appropriate timing, (2) the appropriate assessment tool to prevent the 24 items defined as unprofessional conduct, (3) the possibility of assessment to prevent future unprofessional conduct, and (4) the possibility of implementing an interview to assess professional attributes in the KMLE. The appropriate timing options were the basic medical education (BME) period, in the KMLE, graduate medical education (GME), and continuing professional development (CPD) period. The assessment tool options were written examination, objective structured clinical examination (OSCE), practice observation, and interview.
Data sources/measurement
Before the survey, we analyzed 104 pieces of news published from 2011 to 2019 about doctors’ unprofessional conduct using the Critical Incident Technique (CIT) to determine what the public thinks doctors lack in their professional attributes. CIT is one of the qualitative research methods and refers to collecting direct observational information on human behavior, the circumstances, and the contents of critical incidents for use in problem-solving [8,9].
We categorized 104 news into 24 items of unprofessional conduct of doctors. Based on these categories, we developed a survey questionnaire consisting of 26 nominal scales and 3 open-ended questions. A total of 2 questions asked the reason for the responses and 1 free opinion. To secure content validity, 5 medical educationalists, including medical doctors, developed questionnaires and critically reviewed questionnaires 4 times. No reliability test was conducted due to the descriptive characteristics of the survey tool. A survey questionnaire is presented in Supplement 1.
Bias
To avoid potential sources of bias, we selected all regular members of the Korean Society of Medical Education as respondents. We checked whether there was any discriminatory terminology in 24 types of unprofessional conduct reflected in the questionnaire.
Study size
Since it is not a controlled study, the study size estimation was not possible. Only those who agreed to participate voluntarily were included.
Statistical methods
Descriptive statistics, a cross-tabulation analysis, and Fisher’s exact test were applied to the questionnaire responses using the JAMOVI ver. 2.2.2 program (https://www.jamovi.org). As the expected frequency of fewer than 5 cells accounted for more than 20% of the total cells, the significance probability was confirmed by Fisher’s exact test. The statistical significance was set at 0.05. We analyzed the responses to the open-ended questions using the conventional content analysis method [10]. According to the method, we categorized the responses into keywords. The primary coding and category classification was done by the first author (S.J.N.), and all researchers reviewed the classification content through 3 meetings to ensure content validity.
Results
Participants
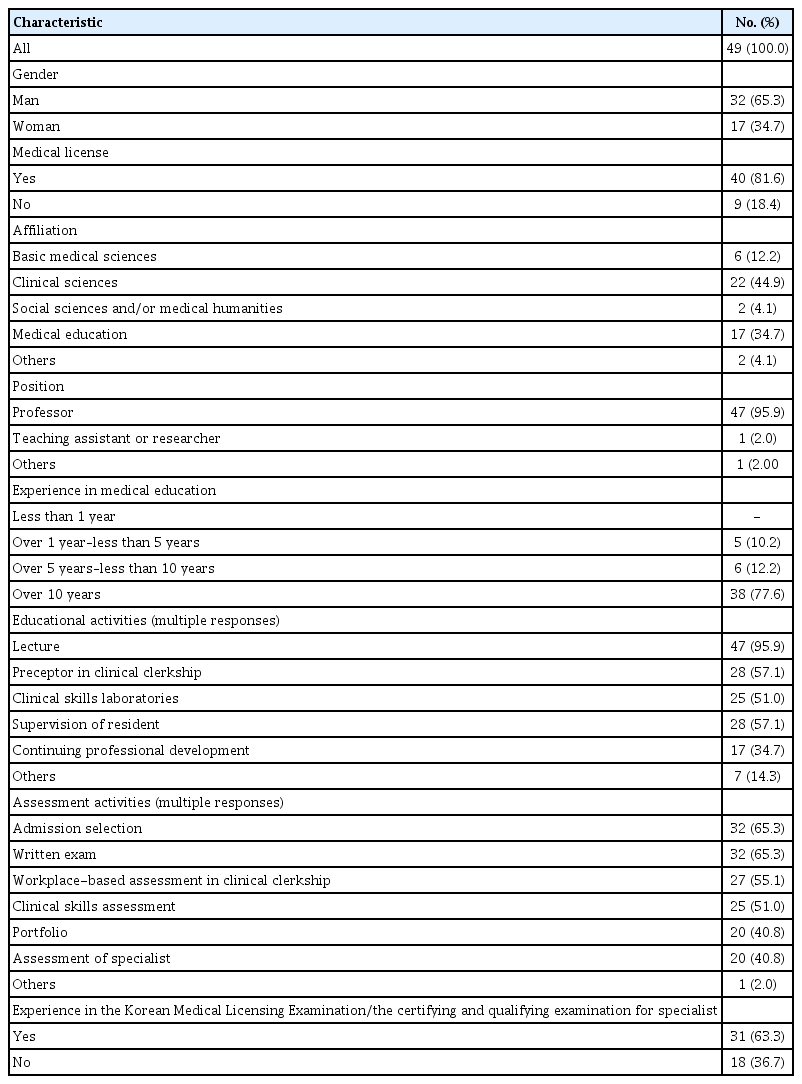
A total of 49 respondents were the subject of the final analysis. Of these, 24 answered the added question of the second survey. Detailed demographic information about the 49 respondents is reported in Table 1. Raw responses data of two surveys are available from Dataset 1.
Respondents’ current state of affairs
Appropriate timing of the assessment to prevent the 24 items of unprofessional conduct
The appropriate timing required to assess 24 items of unprofessional conduct of doctors is presented in Table 2. None of the appropriate timings had an overwhelming response rate for assessing specific unprofessional conduct, except for 2 items. “In the BME” was the dominant timing for 2 items “posting patients’ information on social media” (61.2%), and “sexual assault in the healthcare environment” (55.1%). The average number of respondents who answered was 18.3 (37.4%) in the BME, 15.2 (31.0%) in GME/CPD, 11.5 (23.6%) in the KMLE, and 3.9 (8.0%) suggested no assessment required.

Appropriate assessment time for each unprofessional conduct (N=49)
An appropriate assessment tool to prevent the 24 items of unprofessional conduct
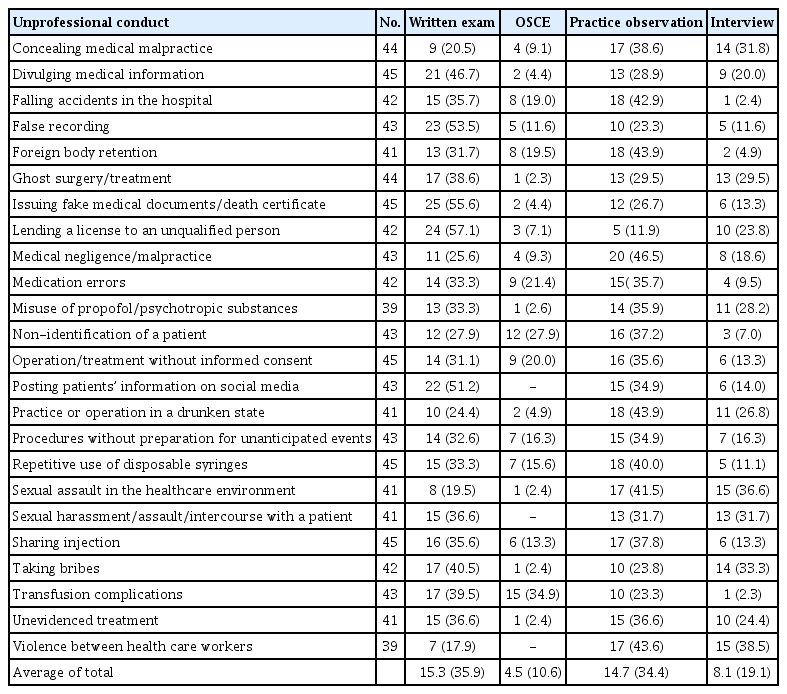
The appropriate assessment tools to prevent the 24 items of unprofessional conduct are presented in Table 3. None of the 4 assessment tools had an overwhelming response rate for assessing specific unprofessional conduct. An average of 15.3 (35.9%) respondents selected a written exam, 14.7 (34.4%) practice observation, 8.1 (19.1%) an interview, and 4.5 (10.6%) OSCE.
Appropriate assessment tool for each unprofessional conduct
Possibility of preventing unprofessional conduct when an interview is introduced to the KMLE
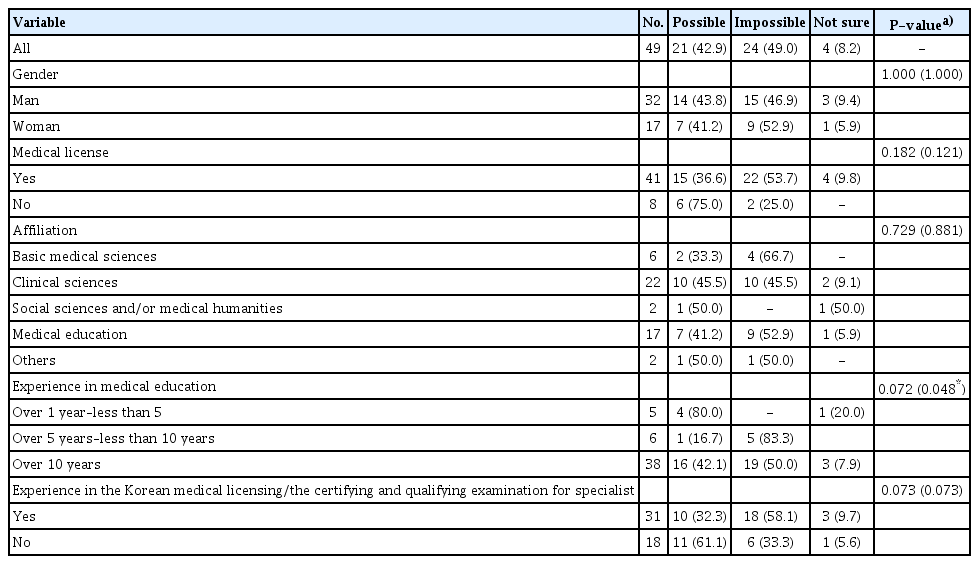
The responses to whether introducing an interview to the KMLE could prevent unprofessional conduct are provided in Table 4. There were slightly more “impossible” (n=24, 49.0%) responses than “possible” (n=21, 42.9%). A total of 24 (63.2%) out of 38 medical educators with more than 5 years of experience answered “impossible.” A total of 4 (80.0%) out of 5 medical educators with less than 5 years of experience answered “possible.” There was a statistically significant difference according to the medical education experience (P=0.048).
Possibility of preventing unprofessional conduct by the introduction of an interview to assess professional attributes
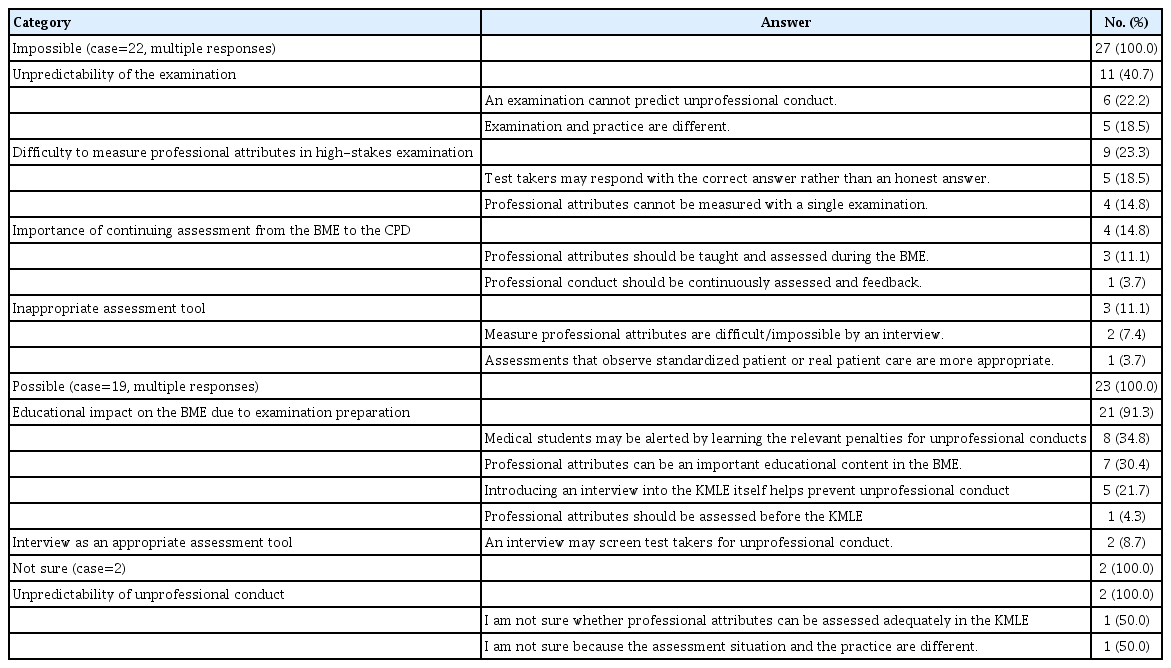
The respondents’ descriptions of the reasons for their thoughts/opinions are presented in Table 5. Of the multiple options, 22 respondents responded “impossible” to 27 items. Those who stated “impossible” said that the examination could not predict unprofessional conduct (n=11, 40.7%), that professional attributes were difficult to measure by licensing examination (n=9, 23.3%), should be assessed continuously from BME to CPD (n=4, 14.8%), and an interview was inappropriate as an assessment tool (n=3, 11.1%).
Analysis of reasons for responses to the possibility of preventing unprofessional conduct
Of the multiple options, 19 respondents responded “possible” to 19 items. The overwhelming response was an impact of emphasizing professional attributes in BME (n=21, 91.3%). There were also responses that an interview was appropriate as an assessment tool (n=2, 8.7%).
Possibility of implementing an interview to assess professional attributes in the KMLE
The responses regarding whether implementing an interview in the KMLE was possible are presented in Table 6. “Impossible” (n=12, 50.0%) was selected more often than “possible” (n=8, 33.3%). There was no statistically significant difference between groups according to demographic characteristics.
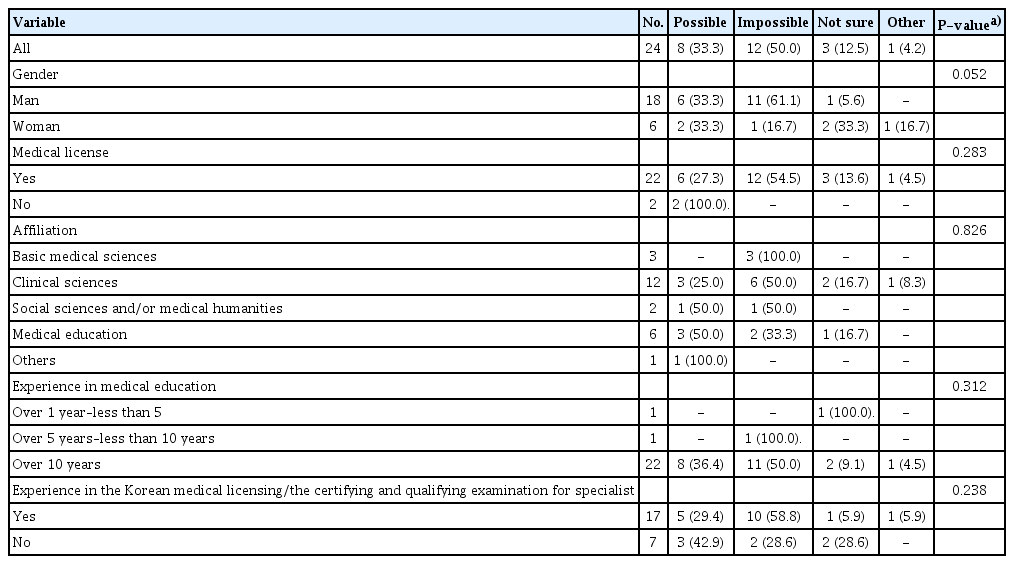
Possibility of implementing an interview to assess professional attributes in the Korean Medical Licensing Examination
The contents of the respondents’ descriptions of the reasons for their thoughts/opinions are provided in Table 7. Respondents who “impossible” said that ensuring the validity, reliability, and objectivity of the interview was difficult (n=5, 50.0%), there was no cost-effectiveness (n=4, 40.0%), and developing assessment questions were difficult (n=1, 10.0%). All respondents who answered “possible” said that implementing an interview depends on the willingness of the examination institution (n=2, 100%).

Analysis of response to the implementation of an interview to assess professional attributes in the Korean Medical Licensing Examination
Discussion
Key results
Medical educators responded evenly to the BME, the KMLE, and GME/CPD at appropriate assessment timing to assess preventing the unprofessional conduct of doctors. Medical educators did not overwhelmingly select an appropriate assessment tool during the written examination, practice observation, an interview, and OSCE. Medical educators responded with “impossible” and “possible” at a similar rate to prevent unprofessional conduct by introducing an interview to the KMLE. However, half of the medical educators answered “impossible” for implementing an interview in the KMLE, and “possible” was even lower.
Interpretation
There was no overwhelming timing to assess doctors’ unprofessional conduct, which may imply that the professional conduct should be continuously assessed during the BME, in the KMLE, and GME/CPD period, not a specific period. This is because professional attributes are not acquired at a specific time but require continuous development. Therefore, the public’s argument that assessing professional attributes in a single test, such as licensing examination, can screen unprofessional doctors does not seem valid.
There was no dominant assessment tool among the 4 assessment tools, which may imply that various tools should be used instead of one specific tool to assess professional attributes. The appropriate tools are different depending on the professional attributes to be evaluated, and using multiple tools, not just one, is important for accurate measurement. This result can be interpreted as not valid for the public argument that an interview is the best tool for assessing professional attributes. Rather than blaming the unprofessional conduct of individual doctors, it seems more appropriate to create a system that continuously educates and assesses professional performance. Therefore, instead of enabling practice throughout a lifetime with a single test such as licensing examination, professional bodies should continuously assess colleagues to ensure they are not engaged in unprofessional conduct.
The response rates of “impossible” and “possible” to prevent unprofessional conduct by introducing an interview in the KMLE were similar. The position of “impossible” focused on whether professional attributes were measurable in the licensing examination and whether an interview could successfully discriminate as an assessment tool. However, the “possible” position seemed to focus on the educational effect that professional attributes are taught as examination content. There was a difference in that “impossible” was selected from a psychometric perspective and “possible” from an educational perspective. It is interesting to note that both the positions of “impossible” and “possible” posit that professional attributes should be important education content in the BME. However, it is known that a downside is that assessment drives learning. There is a risk that medical students focus on the skills they need to achieve high scores. The BME is a very important period in which medical students can develop their professional identity. However, education and assessment in GME/CPD are also emphasized as doctors need to be professional in practice.
Regarding the implementation of an interview to assess professional attributes in the KMLE, “impossible” was selected more than “possible.” The position of “impossible” seemed to consider practical aspects such as questions (or scenario) development, rater recruitment, and rater training for quality control of an interview. The position of “possible” considered policy perspectives such as the willingness of licensing examination administration. However, it seems impossible to develop questions and recruit and train raters to implement interviews with more than 3,000 examinees, only with the willingness of the examination institution.
In Korea, some unprofessional conduct of doctors is subject to criminal punishment. A change is needed to a system that allows doctors to self-regulate as a professional group rather than legal punishment. Therefore, a system should be developed in which professional bodies regulate doctors autonomously.
Comparison with previous studies
Previous studies argued that professional attributes are not acquired all at once, so should be taught and assessed longitudinally even after graduating from medical school, and self-regulation should be implemented as a lifelong practice [4,5].
In meta-analysis studies on professionalism measures, it is necessary to use an appropriate assessment tool for the purpose and target of the assessment [6,7]. Various tools such as self-assessment, direct observation, peer assessment, patients’ opinions, and role model evaluation have been developed and used to measure professional attributes [6].
Professional attributes include affective domains such as attitudes, values, and goals [4]. According to previous studies, the assessment of the affective domain is less reliable than the cognitive domain [3], and thus should be continuously assessed with various tools [4].
In foreign countries such as the Unties States, Canada, United Kingdom, and Australia, professional bodies manage medical licensure, and licenses are renewed according to workplace-based assessment results every 1 to 5 years [11]. The public or colleagues may report members’ unprofessional conduct to professional bodies, and these warn or discipline members according to the results of their own investigation [12,13].
Limitations
This study has a limitation in that the number of medical educators who responded to the survey was small.
Suggestions
In future studies, an academic review from a psychometric perspective is necessary to introduce interviews to assess professional attributes in the medical licensing examination.
Conclusion
More participants said that the introduction of interviews in licensing examinations cannot prevent the unprofessional conduct of doctors, and has no cost-effectiveness. Professional attributes should be continuously taught and assessed over the period from BME to CPD rather than a single test such as licensing examination. However, unprofessional attributes cannot be prevented by education and assessment. Therefore, a system is needed for recertification of medical licenses and self-regulation by the professional body.
Notes
Authors’ contributions
Conceptualization: HRR, SJN, KHC, KHP, DHK. Data curation: SJN, KHP, KHC. Methodology/formal analysis/validation: SJN, HRR, KHC, KHP, DHK. Project administration: HRR, DHK. Funding acquisition: HRR. Writing–original draft: SJN, HRR. Writing–review & editing: SJN, HRR, KHC, KHP, DHK.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
This work is supported by the research grant of the Korea Health Personnel Licensing Examination (2019, RE02-2003-01).
Data availability
Data files are available from Harvard Dataverse: https://doi.org/10.7910/DVN/PWAWYL
Dataset 1. Survey response data coding.
Acknowledgements
None.
Supplementary materials
Data files are available from Harvard Dataverse: https://doi.org/10.7910/DVN/PWAWYL
Supplement 2. Audio recording of the abstract.