United States medical students’ knowledge of Alzheimer disease
Article information
Abstract
Purpose:
A knowledge gap exists between general physicians and specialists in diagnosing and managing Alzheimer disease (AD). This gap is concerning due to the estimated rise in prevalence of AD and cost to the health care system. Medical school is a viable avenue to decrease the gap, educating future physicians before they specialize. The purpose of this study was to assess the knowledge level of students in their first and final years of medical school.
Methods:
Fourteen participating United States medical schools used e-mail student rosters to distribute an online survey of a quantitative cross-sectional assessment of knowledge about AD; 343 students participated. Knowledge was measured using the 12-item University of Alabama at Birmingham AD Knowledge Test for Health Professionals. General linear models were used to examine the effect of demographic variables and previous experience with AD on knowledge scores.
Results:
Only 2.5% of first year and 68.0% of final year students correctly scored ten or more items on the knowledge scale. Personal experience with AD predicted higher knowledge scores in final year students (P= 0.027).
Conclusion:
Knowledge deficiencies were common in final year medical students. Future studies to identify and evaluate the efficacy of AD education programs in medical schools are warranted. Identifying and disseminating effective programs may help close the knowledge gap.
INTRODUCTION
Alzheimer disease (AD) is a growing public health concern, with prevalence expected to reach between 11 and 16 million United States Americans by 2050 [1]. Primary care physicians can play an integral role in recognizing and diagnosing AD through a number of tests assessing cognitive functioning of patients [2]. Ideally, physicians of all specialties would have the knowledge and skills to manage care and communicate with patients in all stages of the disease. However, evidence of a lack of adherence to practice guidelines for diagnosis and management of AD has emerged [3–5]. Adherence to specific care criteria in the dimensions of assessment, treatment, education and support, and safety has been found to be variable, ranging from 9% to 79%, with adherence below 40% for the majority of criteria [3].
One reason for less than optimal care is a lack of knowledge or skills in diagnosis and management of AD. The University of Alabama at Birmingham Alzheimer’s Disease Knowledge Test (UAB ADKT) for health professionals was developed as a brief assessment of knowledge and familiarity regarding AD diagnosis, treatment, and management [6]. Evaluations utilizing this scale showed a significant difference between general physicians and AD specialists [2,6]. Lack of knowledge can delay the diagnosis, in turn delaying treatment and management, and reducing time available for the patient and family members to address legal matters (e.g., living wills, conservatorship, guardianship, etc.).
Healthy People 2020 introduced a novel objective to increase the proportion of AD cases correctly diagnosed with the disease [7]. Decreasing the knowledge gap is one means of achieving this objective. In this study, we examine one avenue to address the physician knowledge gap: future physicians training during their undergraduate medical education.
METHODS
Study design
This was a quantitative cross-sectional survey study design, utilizing the UAB ADKT to assess knowledge related to AD in medical students in their first year of medical school and those in their final year. Medical schools selected for recruitment in this study were comprised of United States allopathic medical schools accredited by the American Association of Medical College who had both first year students and final year students for the 2010–2011 academic school year; total 126 schools, 79 public and 47 private, met inclusion criteria. Fourteen schools (11.1%) agreed to participate in the study, eight schools (6.3%) declined, and another eight schools (6.3%) responded to invitations, but never officially declined nor agreed. The remaining 96 schools (76.2%) did not respond to either correspondence.
Institutions were provided with a standard e-mail invitation to be distributed to medical students enrolled in their first or final year of medical school. The invitation informed students of the purpose and significance of the study and provided a link to the online survey. Medical school representatives were also provided a reminder e-mail to send to students one week after the initial e-mail. The emails to students presented informed consent and continued to the survey, which began with the UAB ADKT and concluded with questions regarding their medical school education, previous personal, volunteer and/or work experience with AD and demographic questions. The survey was administered via Survey Monkey (http://www.surveymonkey.com/), a web-based survey engine. Students were not required to participate in the study during class time and were able to complete the survey at their convenience.
Approval for the study of human subjects was obtained from the Institutional Review Board at San Diego State University. Student scores were collected anonymously. Medical schools were provided the results of their students’ aggregate scores and whether or not these scores were significantly different than the overall average.
University of Alabama at Birmingham Alzheimer’s Disease Knowledge Test
The UAB ADKT consists of twelve multiple-choice questions (Table 1) covering five domains: assessment, clinical course, terminology, legal issues, and patient management [6]. Mean scores in a survey of undergraduate nursing students, general physicians and specialists were found to be 4.76 (SD= 1.86), 8.49 (SD= 2.20) and 10.75 (SD= 1.34), respectively [6]. Question one was slightly altered from “One of the risk factors for Alzheimer’s disease is:” to read “The greatest risk factor for Alzheimer’s disease is:” (Table 1).
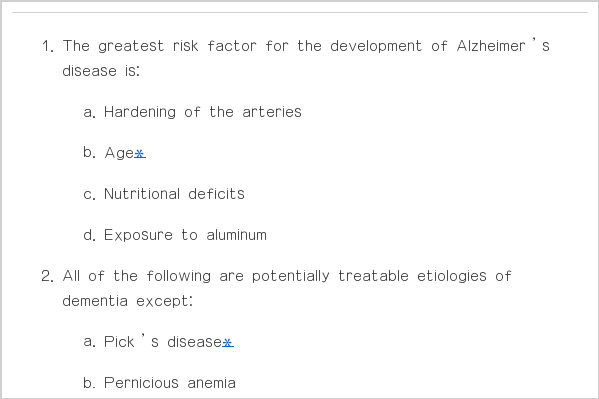
University of Alabama at Birmingham Alzheimer's Disease Knowledge Test for Health Professionals
Statistical methods
Descriptive P-values comparing demographics and the proportion of each test item correctly scored by first year versus final year students were calculated using Fisher exact test. A general linear model was used to investigate factors predicting knowledge scores of final year students. The model analyzed the joint effects of school, advanced age (≥ 28 years), sex, type of specialty (dichotomized as neurology, geriatrics, psychiatry, or geriatric psychiatry versus any other), and type of previous experience with AD on knowledge score. Data were analyzed with the SPSS (SPSS Inc., Chicago IL, USA).
RESULTS
Characteristics of participating medical students
A total of 343 students participated. Demographic characteristics of respondents are summarized in Table 2. First year students accounted for 47.2% (n= 162) of the total sample and final year students comprised the remaining 52.8% (n= 181). Sixty-six first year students (40.7%) and 111 final year students (61.3%) reported any type of previous experience with AD (Table 2).
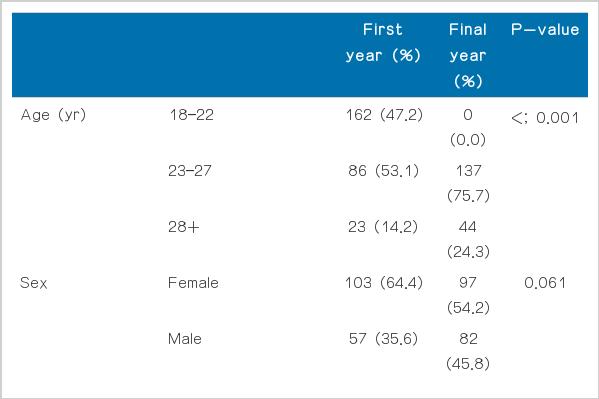
Demographics of 343 medical students from 14 medical schools that agreed to participated in the email survey on the University of Alabama at Birmingham Alzheimer’s Disease Knowledge Test for Health Professionals
UAB ADKT scores
The mean knowledge score was 6.03 (SD = 1.75) for first year students and 10.05 (SD = 1.37) for final year students. Only 2.5% of first year students and 68.0% of final year students scored 10 or more items correctly. The proportion of correct responses for each item is summarized graphically in Fig. 1. Final year students scored significantly better than first year students on all items except item 5, which was scored correctly less than 60% of the time by both first and final year students. Final year students scored well on most of the remaining items, although items 9, 11, and 12 were scored correctly by less than 80% of final year students. In the multivariable analysis of predictors of final year medical student score, only previous personal experience with AD significantly predicted knowledge score (predicting a covariate-adjusted 0.44 point higher score; F[1, 178]= 4.47, P= 0.036).
Comparison of the proportion of correct answers by the first year versus final year students according to items, taken from the email survey with the University of Alabama at Birmingham Alzheimer’s Disease Knowledge Test for Health Professionals, obtained from 343 medical students in 14 medical schools in the United States. *P< 0.05, **P< .001.
DISCUSSION
The primary purpose of this study was to evaluate the knowledge of both first year and final year medical students. We found that first year students were likely to score poorly on the UAB ADKT, with 97.5% scoring 3 or more of the items incorrectly. Final year students on average scored better; nonetheless, nearly one third (32.0%) scored 3 or more items incorrectly. Data were also collected on the students’ previous experiences with AD to examine their role in students’ knowledge. Students with a family member or friend with AD were more likely to perform well on the UAB ADKT.
There are limitations to this study. The participation rate of medical schools was low. Despite an endorsement of our survey from the Alzheimer’s Association’s national chapter, only 14 medical schools agreed to participate. The response rate of medical students was also low within some of the participating schools. We anticipate that students with more knowledge of and experience with AD would be more likely to complete the survey, leading to a positive response bias and possible overestimation of knowledge levels by our survey. This bias is conservative from the perspective of illustrating the need for additional training on AD diagnosis and management; a more representative survey may find an even larger proportion of final year medical students with insufficient knowledge than estimated by our survey. Finally, the 12-question knowledge test was not designed to fully characterize the skill level of students to diagnose and manage AD properly. A more detailed examination may reveal additional relevant deficiencies in knowledge necessary to diagnose and manage AD.
Our findings underscore the importance and need for continuing efforts to improve the training of medical students in anticipation of the growing burden of AD management our health care system is facing. Some medical schools are implementing multidisciplinary courses and clerkships to increase medical students’ experience with geriatric medicine and AD, resulting in students who are more confident in diagnosing and assessing patients for AD with a greater awareness of community resources [8,9]. One novel program pairs first year medical students with patients in the early stages of AD to increase the student’s knowledge of the disease, empathy, and compassion through personal interactions rather than purely clinical contact [10]. These and other efforts to improve the training of the next generation of primary care physicians are to be applauded.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This work was supported by National Institute of Aging grant AG005131.
Supplementary Material: authors’ explanation of their paper in an audio recording of the author speaking or video recording.