Learning styles, academic achievement, and mental health problems among medical students in Thailand
Article information

Abstract
Purpose
This study aimed to investigate the prevalence of various learning styles among medical students and their correlations with academic achievement and mental health problems in these students.
Methods
This study was conducted among 140 first-year medical students of Chiang Mai University, Thailand in 2014. The participants completed the visual-aural-read/write-kinesthetic (VARK) questionnaire, the results of which can be categorized into 4 modes, corresponding to how many of the 4 types are preferred by a respondent. The 10-item Perceived Stress Scale (PSS-10) and the 21-item Outcome Inventory (OI-21) were also used. The participants’ demographic data, grade point average (GPA), and scores of all measurements are presented using simple statistics. Correlation and regression analysis were employed to analyze differences in the scores and to determine the associations among them.
Results
Sixty percent of the participants were female. The mean age was 18.86±0.74 years old. Quadmodal was found to be the most preferred VARK mode (43.6%). Unimodal, bimodal, and trimodal modes were preferred by 35%, 12.9%, and 18.6% of the participants, respectively. Among the strong unimodal learners, visual, aural, read/write, and kinesthetic preferences were reported by 4.3%, 7.1%, 11.4%, and 12.1% of participants, respectively. No difference was observed in the PSS-10, OI-anxiety, OI-depression, and OI-somatization scores according to the VARK modes, although a significant effect was found for OI-interpersonal (F=2.788, P=0.043). Moreover, neither VARK modes nor VARK types were correlated with GPA.
Conclusion
The most preferred VARK learning style among medical students was quadmodal. Learning styles were not associated with GPA or mental health problems, except for interpersonal problems.
Introduction
Learning style is an individual’s characteristic method of gaining knowledge, skills, and attitudes through study or experiences [1]. Among the different models that have been proposed, the visual, aural, read/write, and kinesthetic (VARK) model developed by Neil Fleming is one of the most frequently used methods, and describes preferences in terms of 4 types of preferred learning styles (visual, aural, read/write, and kinesthetic) [2]. Learning preferences are also categorized into 4 modes (unimodal, bimodal, trimodal, and quadmodal), based on the number of learning types preferred. The VARK tool is commonly used by researchers in a variety of disciplines, including medical education.
Studying medicine requires a variety of modes of learning. In previous reports, 56.0% to 86.8% of medical students chose multiple modes of learning. Among the multiple-mode possibilities, 27.6%–43.4% preferred quadmodal learning, and 30.3%–41.0% preferred bimodal learning [3,4,5,6]. Many reports have found unimodal learning to be most prevalent (53.8%–81.9%) [7,8]. Within unimodal learners, aural (21.2%) and kinesthetic (30.1%) were the 2 most preferred VARK styles [3,7,9,10]. Some studies found that the preference of visual and read/write learning styles was associated with gender. However, other studies have reported that VARK results were not associated with gender [7].
Inconsistent findings have been reported regarding the relationship between learning styles and academic achievement [11]. Whether preferred learning styles have an impact on academic achievement among medical students remains unknown. Learning styles and study habits may also predict a medical student’s approaches to and satisfaction with work, stress, and mental health, both when applying to medical school and in the final year. Prior performance may not only predict achievement among students, but also be associated with future achievement at the postgraduate level (i.e., during residency training).
However, the relationships among learning styles, achievement, stress, and mental health require further analysis. To our knowledge, no evidence exists regarding VARK styles, stress, and mental health among medical students. Therefore, our study aimed to explore the prevalence of various learning styles according to the VARK framework among medical students, the correlations between academic achievement and learning styles, and the correlations of stress and mental health problems with the learning styles of these students. Insights about how students learn can result in improved understanding and detection of learners who are at risk of stress-related health problems in medical school.
Methods
Study design and subjects
The study employed a cross-sectional design. A total of 140 of the 250 first-year medical students attending Chiang Mai University were recruited in the 2014 academic year.
Measurement
The measurement tools used included demographic data and grade point average (GPA). Other measures included are listed below.
Thai version of the visual, aural, read/write, and kinesthetic questionnaire version 7.1
VARK is a tool that categorizes learning styles into 4 types (visual, aural, read/write, and kinesthetic). The 4 modes of VARK depend on the number of VARK types chosen (unimodal, bimodal, trimodal, and quadmodal). VARK is commonly used in the education field in a variety of disciplines, including the medical sciences. A Thai version has been made available [12]. The VARK questionnaire contains 16 items, and each has 4 choices reflecting different learning style preferences. More than 1 answer can be endorsed for each item if that matches the participant’s perceptions. The reliability (α) scores of the learning styles are 0.85, 0.82, 0.84, and 0.77 for the visual, aural, read/write, and kinesthetic styles, respectively [13].
Outcome inventory, 21 items
The 21-item outcome inventory (OI-21) is a self-rating questionnaire that measures 4 common mental health problems (depression, anxiety, somatic symptoms, and interpersonal difficulties). The OI-21 contains 21 questions using a 5-choice Likert scale ranging from 1 (never) to 5 (always). The Cronbach α value was found to be 0.92, and its concurrent validity with different measures has been well studied. This tool takes approximately 5–10 minutes to complete [14].
Thai version of the 10-item Perceived Stress Scale
It consists of 10 questions on a 5-choice Likert scale ranging from 0 (never) to 4 (very often), and can be completed within 3–5 minutes. It comprises 2 structures: stress, which is measured by 6 questions, and control, which is measured using 4 questions. The Thai version of 10-item Perceived Stress Scale (PSS-10) had a Cronbach α (total) of 0.85, and an intraclass correlation coefficient of 0.82. Confirmatory factor analysis showed that the goodness-of-fit index was 0.981, the root mean square residual was 0.022, the standardized root mean square residual was 0.037, the comparative fit index was 0.989, the normed fit index was 0.96, the non-normed fit index was 0.981, and the root mean square error of approximation was 0.031 [15].
Statistical analysis
Descriptive statistics was used to analyze the participants’ demographic data, such as gender and age. Analysis of variance was used to compare VARK modes among different GPA, PSS, and OI groups. The predictive power of VARK type on GPA was evaluated using regression analysis. IBM SPSS for Windows ver. 22.0 (IBM Co., Armonk, NY, USA) was used to analyze the data. An α value of 95% was applied throughout.
Ethical approval
Informed consent was obtained from the participants. The study was approved by the Ethics Committee of the Faculty of Medicine, Chiang Mai University, Thailand (IRB no. 004/2015).
Results
Among the 140 participants, the average age was 18.86±0.74 years. The majority (60%) were women. The most prevalent VARK types and modes were kinesthetic (35%) and quadmodal (43.57%) (Fig. 1). Table 1 shows the mean and standard deviation of VARK types and the frequency of VARK modes. No significant differences were observed regarding VARK types or modes between male and female participants. In terms of academic achievement, only the kinesthetic type had a significantly negative correlation with GPA in the first semester (time 1). No significant differences were found between other VARK types, VARK modes, and GPA (Tables 2, 3). No differences were observed among VARK types or modes with regard to the PSS score. No significant differences were found regarding VARK mode and the OI score, except for interpersonal difficulties, for which trimodal participants obtained the highest score. Trimodal learning was associated with significantly higher interpersonal difficulties scores than quadmodal learning (P=0.040) (Tables 4, 5).
Types of visual-aural-read/write-kinesthetic learning styles of 140 first-year medical students of Chiang Mai University, Thailand in 2014.
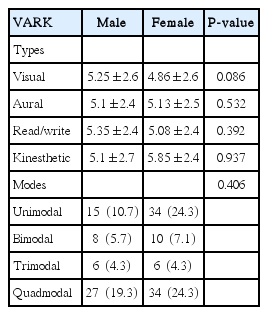
Differences in VARK types and modes according to gender among 140 first-year medical students of Chiang Mai University, Thailand in 2014
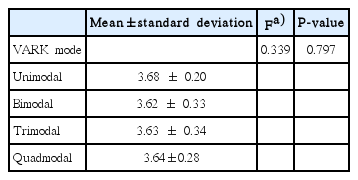
Grade point average according to VARK mode among 140 first-year medical students of Chiang Mai University, Thailand in 2014
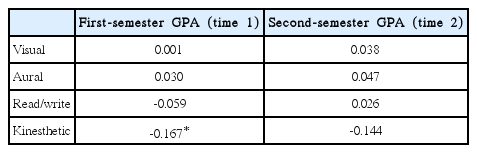
Correlations between visual-aural-read/write-kinesthetic types and grade point average at 2 time points among 140 first-year medical students of Chiang Mai University, Thailand in 2014
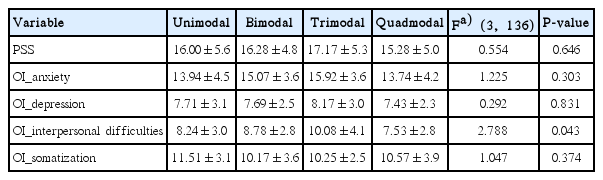
Mean scores of the PSS and OI according to visual-aural-read/write-kinesthetic mode among 140 first-year medical students of Chiang Mai University, Thailand in 2014
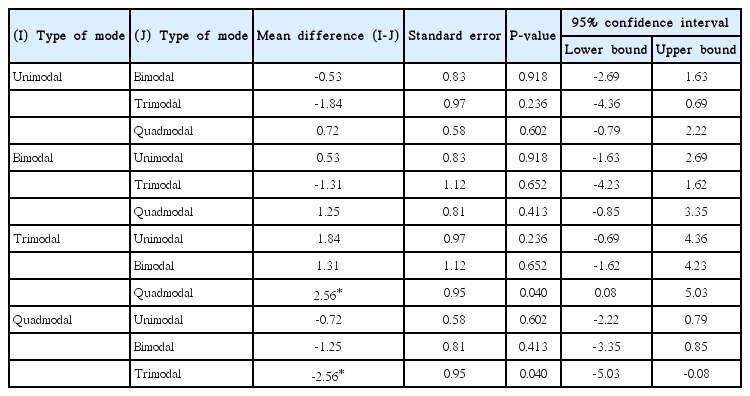
Multiple comparison of visual-aural-read/write-kinesthetic modes concerning interpersonal difficulties among 140 first-year medical students of Chiang Mai University, Thailand in 2014 using post hoc analysis (Tukey honest significant difference)
Discussion
The present study showed that most medical students (65%) had a preference for multimodal VARK learning, which is similar to what has been reported in previous studies. Among these, quadmodal was the most preferred (43.57%) mode of learning. These findings are similar to those of previous studies that reported multiple modes to be the most preferred learning style, with quadmodal learning being the most prevalent among first-year or preclinical students [3,4], while Baykan and Nacar [5] and Prithishkumar and Michael [6] reported that bimodal was the most preferred VARK mode. The authors conjecture that culture and curriculum may contribute to these discrepancies. Our findings imply that medical students preferred their instructors to use different methods of teaching to ensure effective learning. Although the students’ learning preferences were not associated with variations in learning outcomes, providing opportunities to express these abilities and skills may result in success.
In terms of VARK types among individuals who preferred unimodal learning, kinesthetic was the most common learning style. The finding that the visual learning style was found the least preferred type in this study is in line with previous reports [3,4]. The reason that students did not prefer visual learning is unknown, although it constitutes 1 of the 4 required skills for clinical examinations (inspection, palpation, percussion, and auscultation). This may reflect the fact that the participants were surveyed while they were in their first year of medical school. Visual strategies may be least used at that stage of learning because the curriculum design of the first year differs from that of higher levels, especially clinical years where visual ability is required for activities such as using a microscope in histology or pathology classes, investigating structures in anatomy class, examining patients in the clinical years, and so on. This finding may assist curriculum developers in designing a preparatory course for students to enhance their visual strategies in the early years of study. Academic achievement, as defined by GPA, was not related to VARK mode. This finding is consistent with the results reported by Almigbal [7].
In general, achievement outcomes differ in many details, with examples including paper examination scores and rankings, laboratory scores, group assignments or reports, objective structured clinical examinations, and so on. GPA, as a representative measure of academic achievement, may not be sensitive enough to show the differences among VARK learning styles. Therefore, the authors do not recommend that GPA should be used as the only outcome measure for academic achievement. Interestingly, the kinesthetic learning style was found to be negatively related to GPA. This might be because among preclinical students, more time was spent on lectures and learning theories than in practical learning due to the design of the curriculum.
While modes of VARK learning were not associated with perceived stress, anxiety, depression, or somatization, individuals who preferred trimodal VARK learning reported higher scores on the interpersonal difficulties subscale than others. Since insufficient information is available to explain this relationship, further study of this issue might be encouraged. In addition, repeated outcomes and longitudinal monitoring may be warranted.
In conclusion, the most preferred learning style among medical students was quadmodal. Learning styles were not associated with academic achievement or mental health. However, the trimodal learning style was associated with interpersonal problems.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
This study was supported by a research grant of Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand in 2014.