Correlation of burnout syndrome with specific coping strategies, behaviors, and spiritual attitudes among interns at Yale University, New Haven, USA
Article information

Abstract
Purpose:
This study aimed to determine the correlation of burnout syndrome with specific coping strategies, behaviors, and spiritual attitudes among interns in internal medicine, primary care, and internal medicine/pediatrics residency programs at two institutions.
Methods:
Intern physicians completed anonymous voluntary surveys prior to starting the internship in June 2009 and in the middle of the internship in February 2010. Three validated survey instruments were used to explore burnout, coping, and spiritual attitudes: the Maslach Burnout Inventory, the COPE Inventory, and the Hatch Spiritual Involvement and Beliefs Scale. The interns were in programs at the Yale University School of Medicine and a Yale-affiliated community hospital, New Haven, Connecticut, USA.
Results:
The prevalence of self-identified burnout prior to starting the internship was 1/66 (1.5%) in June 2009, increasing to 10/53 (18.9%) in February 2010 (P<0.0001). From June 2009 to February 2010, the prevalence of high emotional exhaustion increased from 30/66 (45.5%) to 45/53 (84.9%) (P<0.0001), and that of high depersonalization increased from 42/66 (63.6%) to 45/53 (84.9%) (P=0.01). Interns who employed the strategies of acceptance and active coping were less likely to experience emotional exhaustion and depersonalization (P<0.05). Perceptions of high personal accomplishment was 75.5% and was positively correlated with total scores on the Hatch Spiritual Involvement and Beliefs Scale, as well as the internal/fluid and existential/meditative domains of that instrument. Specific behaviors did not impact burnout.
Conclusion:
Burnout increased during the intern year. Acceptance, active coping, and spirituality were correlated with less burnout. Specific behaviors were not correlated with burnout domains.
INTRODUCTION
Residency is an arduous period marked by emotional, personal, and intellectual challenges experienced while contending with human suffering. Internship, in particular, is a uniquely challenging experience that can have a profound effect on stress and burnout, as a physician transitions from the role of student to autonomous provider. Several studies have evaluated the prevalence of burnout among resident physicians, finding correlations between burnout and depression [1], providing suboptimal care, and committing more medical errors [2]. Rosen et al. [3] showed that high-level burnout among interns increased from 4.3% at the beginning of the year to 55.3% at year-end (P<0.0001). Changes in duty hours, mandated by the Accreditation Council for Graduate Medical Education, were hoped to reduce the prevalence of exhaustion and improve patient safety. However, the impact of duty hour mandates has been equivocal to neutral [4]. Models for fostering a healthy work-life balance have been proposed, such as training students and residents in healthy adaptive coping strategies [5], addressing institutional culture [6], and seeking to balance professional and personal demands [7]. While these models have been proposed, several factors potentially impacting burnout have not been studied, especially emotional coping strategies and spirituality among interns. Many factors are outside the control of interns, including the call schedule, daily work demands, and team structure. A study that assessed spirituality among residents showed a protective effect of spirituality against depression and burnout [8]. Identifying constructive coping strategies that interns, in particular, employ to protect themselves against burnout may be helpful for reducing errors and improving intern satisfaction. This study aims to identify how specific coping strategies, behaviors, and spiritual attitudes affect burnout among interns in the internal medicine, primary care, and internal medicine/pediatrics residency programs at the Yale University School of Medicine and a Yale-affiliated community hospital internal medicine program at the beginning and middle of the intern year.
METHODS
Study design and sample
We asked intern physicians to complete an anonymous, confidential, and voluntary survey exploring burnout, coping, and spiritual attitudes. We surveyed preliminary and categorical interns from the Yale University internal medicine (n=44), primary care medicine (n=19) and internal medicine/pediatrics (n=4) training programs during the intern orientation in June 2009. In February 2010, we repeated the survey during regularly scheduled inpatient and ambulatory conferences. Interns anonymously returned surveys to either a member of the support staff or placed surveys in an unmarked envelope in their respective conference rooms. A third party, not associated with the survey, entered all data into a spreadsheet for further analysis.
Ethical approval
The Yale University School of Medicine Human Investigations Committee approved the study protocol.
Survey instrument
The survey contained demographic data and three validated instruments: the Maslach burnout inventory (MBI) [9], The comprehensive older persons’ evaluation (COPE) inventory [10], and the Hatch Spiritual Involvement and Beliefs Scale (SIBS) [11]. The MBI is the most commonly used instrument to evaluate burnout among healthcare professionals. The MBI contains 22 items that address three domains of burnout: emotional exhaustion, depersonalization, and personal accomplishment. Each item is scored on a seven-point scale (1=never, 2=a few times a year, 3=once a month or less, 4=a few times a month, 5=once a week, 6=a few times a week, and 7=every day). Standard cutoffs of high, moderate, and low scores are delineated for each domain.
The COPE inventory comprises 15 four-item scales that assess a variety of coping strategies, including adaptive and maladaptive strategies. Participants indicate how frequently they use each coping strategy on a four-point scale anchored by ‘usually do not do this at all’ and ‘usually do this a lot.’ The COPE inventory was specifically designed to evaluate an individual’s responses to a stressful environment. Based on both a theoretical and empirical model, the COPE inventory incorporates both ‘problem-focused’ and ‘emotion-focused’ coping strategies and addresses the deficiencies of prior instruments.
The SIBS instrument investigates broad aspects of spirituality. The SIBS is based on an expansive definition of spirituality as one’s relationship with the divine. The SIBS acknowledges that spirituality incorporates both attitudes and practice, and correlates strongly with other instruments that assess spirituality. It consists of 26 questions on a five-point Likert scale, where 1=strongly agree and 5=strongly disagree. The questions address the broadest aspects of spirituality: ‘internal beliefs,’ such as one’s conception of God; ‘external practices,’ including how often one worships; ‘personal humility,’ which is a relational quality; and ‘existential beliefs,’ including the nature of a ‘spiritual force that influences my life.’ The SIBS also uses language that is not specific to the Judeo-Christian tradition, which is important given the diverse backgrounds of the targeted interns.
Statistical analyses
We used JMP ver. 4.04 (SAS, Cary, NC, USA) for all statistical analyses. We calculated the composite scores of the MBI, COPE, and SIBS instruments. We used the Student t-test and the chi-square test to compare the means of MBI categories with demographic variables and behaviors. Continuous variables were correlated with the Spearman rank coefficient. Multivariate regression modeling was also employed to ascertain the impact of spirituality and coping upon the burnout domains.
RESULTS
Respondent characteristics
In the summer, 66 of 67 (98.5%) interns returned the surveys. In the winter, 53 of 76 (69.7%) interns completed surveys. In July, the average age of the respondents was 28±3 years; 27 (40.9%) were male, 20 (30.4%) were married, six (9.1%) had children, and 36 (54.6%) had spent time off prior to medical school. Comparing the summer and winter time points, no differences existed in gender, age, marital status, parenthood, ethnicity, or having taken time off prior to medical school.
Burnout
The prevalence of self-identified burnout in June prior to starting the internship was 1/66 (1.5%). In February 2010, the prevalence of self-identified burnout rose to 10/53 (18.9%) (P<0.0001). Between June 2009 and February 2010, the prevalence of high emotional exhaustion increased from 30/66 (45.5%) to 45/53 (84.9%) (P<0.0001), and that of high depersonalization increased from 42/66 (63.6%) to 45/53 (84.9%) (P=0.01). The prevalence of low personal satisfaction showed no significant change. Of note, high personal satisfaction also was unchanged between the summer (50/66 [75.8%]) and the winter (40/53 [75.5%]). The prevalence of burnout among the three training programs did not differ. No differences were found in emotional exhaustion, depersonalization, or personal accomplishment based on gender, marital status, the presence of children, or having taken time off prior to medical school.
Intern behaviors
Concrete behaviors such as reading outside the field of medicine, regular exercise, and taking time for family did not demonstrate a protective effect for any burnout domain (Table 1).

Results of the Maslach Burnout Inventory survey in summer 2009 and winter 2010, administered to interns at Yale University, New Haven, USA
Coping strategies
Several coping strategies appeared to be protective against burnout; namely, residents who employed the strategies of acceptance and active coping had lower emotional exhaustion and depersonalization (Table 2). Residents who employed self-blaming, denial, or disengagement had higher emotional exhaustion and depersonalization scores. Interestingly, humor was associated with increased emotional exhaustion (R2=0.33, P=0.03) and depersonalization (R2=0.37, P=0.01). No emotional coping strategy was associated with the domain of personal accomplishment (Table 2).
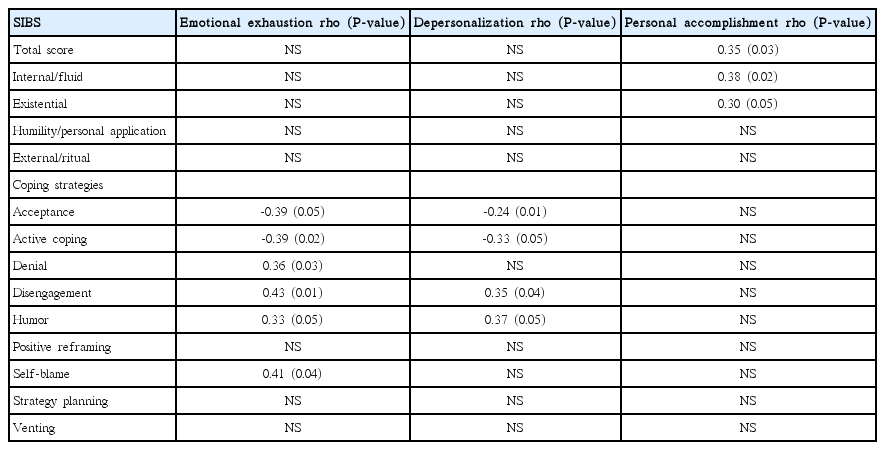
Spearman rank correlations between burnout domains, spirituality, and emotional coping among interns in February 2010 in Yale University, New Haven, USA
Spirituality
Table 2 shows correlations between the SIBS score and the burnout domains. Personal accomplishment was positively correlated with the SIBS total score, as well as the internal/fluid and existential axes. Otherwise, the SIBS score did not impact emotional exhaustion or depersonalization. Multivariate regression revealed that the SIBS inventory and the emotional coping measurements accounted for 65% of the variance for emotional exhaustion (P=0.003), and 70% of the variance for depersonalization (P=0.0006). The impact of SIBS and emotional coping upon personal accomplishment was not significant (R2=0.40, P=0.32). However, SIBS alone was significantly associated with personal accomplishment (R2=0.15, P=0.007).
DISCUSSION
Our data reveal several intriguing findings about coping, burnout, and spirituality among physicians facing the difficult challenges of internship. First, upon arrival to internship, 30 (45%) met the criteria for high emotional exhaustion and 42 (64%) met the criteria for high depersonalization. These findings are quite different from those of Rosen et al., who reported a much lower prevalence of 4.3% [3]. Our data suggest a residual impact from the experience of medical school and raises several questions. What is it about the curriculum and culture of medical school that results in the high prevalence of intern burnout ‘even prior to starting residency?’ Is the high prevalence of depersonalization a coping strategy, a distancing, from the emotional stress of learning medicine? Must residency programs address burnout earlier in the training process? Although many interns started residency with symptoms of burnout, the prevalence increased during the winter months. However, our findings demonstrated heterogeneous manifestations of burnout. Emotional exhaustion (84.9%), depersonalization (84.9%), and personal accomplishment (75.5%) were observed to have a high prevalence. Despite the workload and the ensuing tendency for objectification, interns still have a sense that their work has meaning and purpose. This finding highlights the heterogeneous nature of burnout, where the three variables sometimes do not correlate tightly. An intern may experience not only some aspects of burnout, especially emotional exhaustion due to the demands of the job or depersonalization to distance oneself from the suffering of patients, but also a high degree of professional satisfaction about the impact made upon patients’ lives.
Second, we speculated that interns who engaged in activities outside the hospital or participated in extracurricular activities, such as research projects, would suffer less burnout. For example, participating in extracurricular activities would reflect an abiding interest, giving meaning and context to their role as interns and allowing them to incorporate varied experiences into their daily tasks. Moreover, extracurricular activities could reflect time management skills, mentorship seeking, and more interpersonal relationships. The data, however, did not support this hypothesis; although we speculated that extracurricular activities might be negatively correlated with burnout, no significant correlation was found (Table 2). While extracurricular involvement has not been studied among residents, a study among parish-based clergy demonstrated that varied activities, both within and outside one’s vocation, were associated with a lower prevalence of burnout [12].
Third, several emotional coping strategies had either a significantly helpful or harmful impact on emotional exhaustion and depersonalization. Acceptance and active coping were strongly associated with lower emotional exhaustion and depersonalization. Conversely, self-blame, denial, disengagement, and humor were associated with higher emotional exhaustion and depersonalization. Acceptance and active coping are proactive, self-reflective strategies that suggest a certain maturity. “I accept the reality of what has happened” and “I concentrate my efforts on doing something about it” are items that imply thoughtful introspection. Conversely, self-blame, denial, and disengagement are reactive, emotionally raw responses to stress. These findings are similar to those of the study of Sevencan et al. [13] dealing with burnout among interns and affirm the importance of emotional maturity and positive coping skills in mitigating burnout.
Fourth, spirituality also impacted burnout, most notably the internal/fluid and existential/meditative domains of the SIBS. The internal/fluid domain explores a person’s belief system, rather than their attendance or participation in formal religion. “My life has a purpose,” “My spiritual beliefs continue to evolve,” and “I can find meaning in times of hardship” are examples of internal belief items that suggest both flexibility and purpose in one’s belief system. The meditative/existential domain complements the internal/fluid system, with a focus on the belief in the utility of prayer and meditation. Interns with higher scores in the internal/fluid domain and the existential/meditative domain had a greater sense of personal accomplishment. However, those scores did not impact emotional exhaustion or depersonalization. The beliefs reflected in those items perhaps give support and meaning to the daily chores of patient care, thereby impacting personal accomplishment. However, these same beliefs are not enough to mitigate the intense physical demands and reflexive objectification that comes with the complicated nature of patient care. Other studies have evaluated correlations between spirituality and burnout among medical residents and students [1,2,13]. However, two of those studies did not distinguish which aspects of spirituality were relevant to the various burnout domains [2,13]. Among this intern population, where the prevalence of burnout was high, attendance at religious services or private religious practices was not found to be significantly associated with burnout. Instead, the internal and existential qualities of faith (items assessing ‘purpose’ and ‘meaning in times of hardship’) were found to be significant. The overt practice of religion was not found to have a statistically significant effect.
Some limitations of this study should be considered. First, with the exception of the community hospital program, all interns rotated within one training system. This shared experience opens the study to selection bias, because some unique features of the Yale experience may have promoted or protected against burnout. Nevertheless, the interns came from a multitude of different medical schools and personal backgrounds that should have influenced them as much, if not more, than their current training environment. Second, this study assessed correlations between data, but does not imply causation. Burnout, depression, and coping may reflect a continuum of varied responses to stress rather than separate variables that influence each other.
In conclusion, we found that interns who employed specific strategies of acceptance, active coping, and spiritual attitudes had lower levels of burnout. Despite this, behaviors such as reading outside the field of medicine, regular exercise, and taking time for family did not lessen any aspect of burnout. Recognizing the specific factors that may influence burnout may help program directors and interns mitigate the negative effects of training.
Notes
No potential conflict of interest relevant to the study was reported.
SUPPLEMENTARY MATERIAL
Audio recording of the abstract.